| pA2 online © Copyright 2004 The British Pharmacological Society |
179P
University of Newcastle Winter Meeting December 2004 |
Investigation of the forearm vascular effects of inhaled tiotropium T. Attinà, J. J. Oliver & D. J. Webb.Clinical Pharmacology Unit & Research Centre, The University of Edinburgh, Edinburgh, Scotland, UK. |
|
Tiotropium is a recently introduced anti-muscarinic, bronchodilator drug, which is an effective treatment for chronic obstructive pulmonary disease [1]. Tiotropium has approximately equal affinity for each of the five known muscarinic receptor subtypes but dissociates slowly from the M1 and M3 subtypes. Its action is, therefore, relatively M1- and particularly M3-specific. Systemic anticholinergic effects of inhaled tiotropium have been reported from clinical trials. However, the potential systemic vascular effects of local administration to the lung have not been investigated in detail. Acetylcholine (ACh) is a muscarinic agonist that causes vasodilatation in the forearm when infused at the brachial artery. It is not entirely clear which receptor subtypes mediate this effect, although indirect evidence suggests that the M3 subtype is important [2].
On the basis of the results of a previous study, in which we assessed the systemic vascular effects of acute administration of tiotropium, we now investigated the effects of a 1-week treatment with inhaled tiotropium on the dose response curve of ACh-mediated vasodilatation in the forearm.
Ten healthy subjects (males) were studied in a two-way, randomized, placebo-controlled, single-blind, crossover study. They received 1-week treatment with either tiotropium 18 m g (as Spiriva, using the commercially available HandiHaler® device) or placebo once daily. On the 2 study days, the brachial artery of the non-dominant arm of each subject was cannulated with a 27-SWG cannula, under local anaesthesia and, after a 30 min saline infusion (1ml min-1) and baseline forearm blood flow (FBF) measurements [3], ACh was infused for 6 min at five different doses (0.6, 2, 6, 20 and 60 µg min-1). FBF was then assessed during the last 3 min of each dose. Also, in a subgroup of five subjects, we assessed the response to ACh after the intra-arterial infusion of the non-selective muscarinic antagonist atropine as an active control. Differences between tiotropium and placebo in the responses to different doses of ACh were compared by Student’s t-test (Excel v5.0, Microsoft). Statistical significance was taken at the 5% level.
The forearm vascular response to ACh (0.6, 2, 6, 20 and 60 µg min-1) was not significantly different between tiotropium and placebo (Figure 1).
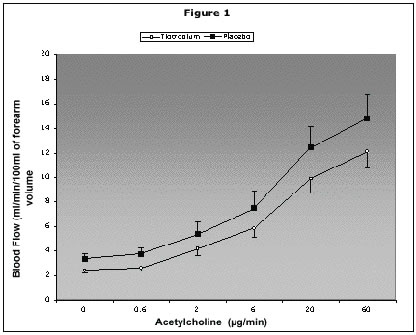
Treatment for 1 week with tiotropium did not affect the response to ACh in the forearm vasculature.
This result may suggest that neither the M1 nor the M3 receptor subtype mediate cholinergic vasodilatation in the forearm.
1. Hvizdos KM, Goa KL. Drugs 2002; 62: 1195.
2. Bruning TA, et al. Circ Res 1994; 74: 912.
3. Wilkinson IB, Webb DJ. Br J Clin Pharmacol 2001; 52: 631.